Skip to content
Healthy
Charles County
Facebook
Facebook-f
Twitter
Youtube
Home
COVID
COVID-19 Vaccinations
Adult Immunization
Child Immunization
Testing
At home testing kits
COVID-19 Testing
Local covid-19 data
My Community
Event Request Form
Employment
Food Resources
Health For All Coalition – Disability Inclusion
Internships
Local Health Improvement Coalition
Notice of Privacy Practices
Public Health
Reports and Summaries
Resources
Social Media Presence
CCDoH Facebook
CCDoH Twitter
Healthy Charles County
Partnerships for a Healthier Charles County
Tobacco and Cancer Coalition
Volunteers
Walk Charles County
Walking Map
Walking Action Plan
Walking Guide
Services
(ACC) / Ombudsman Program
Adult Evaluation
Asthma & Lead Poisoning Prevention
Babies Born Healthy
Car Seat Checks
Childbirth Class
Behavioral Health
Mental Health Services
Grief and Loss Therapeutic Group
Suicide Prevention
Smoking Cessation
E-Cigarettes/Vaping
Substance Use Services
Birth Certificates
Home Births
Cancer Screening and Prevention
Chronic Disease
Building Better Caregivers
Diabetes Prevention Program
Chronic Disease Self Management Workshop
Healthy Hearts Start at Home
Death Certificates
Dental Health
Disability Services
Emergency Preparedness
Family Planning
HIV Services
Immunization
Adult
Child
Infants and Toddlers
Infectious Diseases
Maryland Children Health Insurance Program (MCHP)
Non Emergency Medical Transportation Program (NEMT)
Menthol Information
PrEP
School Health
Sexually Transmitted Infection (STI)
Tobacco Cessation
Women, Infants & Children (WIC)
Environmental Health
Animal Health & Safety
Animal Health Resources
Rabies
Exotic Birds
Bats in Home
Animals in Public Settings
Snake Bite prevention Tips
Applications
Sanitary Survey Request
Bed Bug Resources
Complaint Form
Food Safety
Providers
Indoor Air Quality
Mold Resources
Radon
Notice of Right to Appeal
Food Service Facility
Well and Septic
Percolation/Sewage/Bay Restoration
Request for Property Information
Temporary Events
LBHA
Naloxone and the Overdose Response Program
Education
Building Better Caregivers
Healthy Eating
Hypertension
Cholesterol
Child Safety Seats
Diabetes
Disability Inclusion
Fall Prevention
Let’s Live Well Health Guide
Prediabetes
TOPS
Trauma Informed Care
Walking
Health Professionals
(COMAR) Reportable Diseases
COVID Vaccine Communication Resources for Pediatricians
CDC Health Advisory – Outbreak of Pseudomonas aeruginosa
Health Alert Network
Human Parechovirus (PeV)
Maryland Morbidity Report Form
Measles Vaccinations
Tuberculosis
Menu
Home
COVID
COVID-19 Vaccinations
Adult Immunization
Child Immunization
Testing
At home testing kits
COVID-19 Testing
Local covid-19 data
My Community
Event Request Form
Employment
Food Resources
Health For All Coalition – Disability Inclusion
Internships
Local Health Improvement Coalition
Notice of Privacy Practices
Public Health
Reports and Summaries
Resources
Social Media Presence
CCDoH Facebook
CCDoH Twitter
Healthy Charles County
Partnerships for a Healthier Charles County
Tobacco and Cancer Coalition
Volunteers
Walk Charles County
Walking Map
Walking Action Plan
Walking Guide
Services
(ACC) / Ombudsman Program
Adult Evaluation
Asthma & Lead Poisoning Prevention
Babies Born Healthy
Car Seat Checks
Childbirth Class
Behavioral Health
Mental Health Services
Grief and Loss Therapeutic Group
Suicide Prevention
Smoking Cessation
E-Cigarettes/Vaping
Substance Use Services
Birth Certificates
Home Births
Cancer Screening and Prevention
Chronic Disease
Building Better Caregivers
Diabetes Prevention Program
Chronic Disease Self Management Workshop
Healthy Hearts Start at Home
Death Certificates
Dental Health
Disability Services
Emergency Preparedness
Family Planning
HIV Services
Immunization
Adult
Child
Infants and Toddlers
Infectious Diseases
Maryland Children Health Insurance Program (MCHP)
Non Emergency Medical Transportation Program (NEMT)
Menthol Information
PrEP
School Health
Sexually Transmitted Infection (STI)
Tobacco Cessation
Women, Infants & Children (WIC)
Environmental Health
Animal Health & Safety
Animal Health Resources
Rabies
Exotic Birds
Bats in Home
Animals in Public Settings
Snake Bite prevention Tips
Applications
Sanitary Survey Request
Bed Bug Resources
Complaint Form
Food Safety
Providers
Indoor Air Quality
Mold Resources
Radon
Notice of Right to Appeal
Food Service Facility
Well and Septic
Percolation/Sewage/Bay Restoration
Request for Property Information
Temporary Events
LBHA
Naloxone and the Overdose Response Program
Education
Building Better Caregivers
Healthy Eating
Hypertension
Cholesterol
Child Safety Seats
Diabetes
Disability Inclusion
Fall Prevention
Let’s Live Well Health Guide
Prediabetes
TOPS
Trauma Informed Care
Walking
Health Professionals
(COMAR) Reportable Diseases
COVID Vaccine Communication Resources for Pediatricians
CDC Health Advisory – Outbreak of Pseudomonas aeruginosa
Health Alert Network
Human Parechovirus (PeV)
Maryland Morbidity Report Form
Measles Vaccinations
Tuberculosis
Home
COVID
COVID-19 Vaccinations
Adult Immunization
Child Immunization
Testing
At home testing kits
COVID-19 Testing
Local covid-19 data
My Community
Event Request Form
Employment
Food Resources
Health For All Coalition – Disability Inclusion
Internships
Local Health Improvement Coalition
Notice of Privacy Practices
Public Health
Reports and Summaries
Resources
Social Media Presence
CCDoH Facebook
CCDoH Twitter
Healthy Charles County
Partnerships for a Healthier Charles County
Tobacco and Cancer Coalition
Volunteers
Walk Charles County
Walking Map
Walking Action Plan
Walking Guide
Services
(ACC) / Ombudsman Program
Adult Evaluation
Asthma & Lead Poisoning Prevention
Babies Born Healthy
Car Seat Checks
Childbirth Class
Behavioral Health
Mental Health Services
Grief and Loss Therapeutic Group
Suicide Prevention
Smoking Cessation
E-Cigarettes/Vaping
Substance Use Services
Birth Certificates
Home Births
Cancer Screening and Prevention
Chronic Disease
Building Better Caregivers
Diabetes Prevention Program
Chronic Disease Self Management Workshop
Healthy Hearts Start at Home
Death Certificates
Dental Health
Disability Services
Emergency Preparedness
Family Planning
HIV Services
Immunization
Adult
Child
Infants and Toddlers
Infectious Diseases
Maryland Children Health Insurance Program (MCHP)
Non Emergency Medical Transportation Program (NEMT)
Menthol Information
PrEP
School Health
Sexually Transmitted Infection (STI)
Tobacco Cessation
Women, Infants & Children (WIC)
Environmental Health
Animal Health & Safety
Animal Health Resources
Rabies
Exotic Birds
Bats in Home
Animals in Public Settings
Snake Bite prevention Tips
Applications
Sanitary Survey Request
Bed Bug Resources
Complaint Form
Food Safety
Providers
Indoor Air Quality
Mold Resources
Radon
Notice of Right to Appeal
Food Service Facility
Well and Septic
Percolation/Sewage/Bay Restoration
Request for Property Information
Temporary Events
LBHA
Naloxone and the Overdose Response Program
Education
Building Better Caregivers
Healthy Eating
Hypertension
Cholesterol
Child Safety Seats
Diabetes
Disability Inclusion
Fall Prevention
Let’s Live Well Health Guide
Prediabetes
TOPS
Trauma Informed Care
Walking
Health Professionals
(COMAR) Reportable Diseases
COVID Vaccine Communication Resources for Pediatricians
CDC Health Advisory – Outbreak of Pseudomonas aeruginosa
Health Alert Network
Human Parechovirus (PeV)
Maryland Morbidity Report Form
Measles Vaccinations
Tuberculosis
Menu
Home
COVID
COVID-19 Vaccinations
Adult Immunization
Child Immunization
Testing
At home testing kits
COVID-19 Testing
Local covid-19 data
My Community
Event Request Form
Employment
Food Resources
Health For All Coalition – Disability Inclusion
Internships
Local Health Improvement Coalition
Notice of Privacy Practices
Public Health
Reports and Summaries
Resources
Social Media Presence
CCDoH Facebook
CCDoH Twitter
Healthy Charles County
Partnerships for a Healthier Charles County
Tobacco and Cancer Coalition
Volunteers
Walk Charles County
Walking Map
Walking Action Plan
Walking Guide
Services
(ACC) / Ombudsman Program
Adult Evaluation
Asthma & Lead Poisoning Prevention
Babies Born Healthy
Car Seat Checks
Childbirth Class
Behavioral Health
Mental Health Services
Grief and Loss Therapeutic Group
Suicide Prevention
Smoking Cessation
E-Cigarettes/Vaping
Substance Use Services
Birth Certificates
Home Births
Cancer Screening and Prevention
Chronic Disease
Building Better Caregivers
Diabetes Prevention Program
Chronic Disease Self Management Workshop
Healthy Hearts Start at Home
Death Certificates
Dental Health
Disability Services
Emergency Preparedness
Family Planning
HIV Services
Immunization
Adult
Child
Infants and Toddlers
Infectious Diseases
Maryland Children Health Insurance Program (MCHP)
Non Emergency Medical Transportation Program (NEMT)
Menthol Information
PrEP
School Health
Sexually Transmitted Infection (STI)
Tobacco Cessation
Women, Infants & Children (WIC)
Environmental Health
Animal Health & Safety
Animal Health Resources
Rabies
Exotic Birds
Bats in Home
Animals in Public Settings
Snake Bite prevention Tips
Applications
Sanitary Survey Request
Bed Bug Resources
Complaint Form
Food Safety
Providers
Indoor Air Quality
Mold Resources
Radon
Notice of Right to Appeal
Food Service Facility
Well and Septic
Percolation/Sewage/Bay Restoration
Request for Property Information
Temporary Events
LBHA
Naloxone and the Overdose Response Program
Education
Building Better Caregivers
Healthy Eating
Hypertension
Cholesterol
Child Safety Seats
Diabetes
Disability Inclusion
Fall Prevention
Let’s Live Well Health Guide
Prediabetes
TOPS
Trauma Informed Care
Walking
Health Professionals
(COMAR) Reportable Diseases
COVID Vaccine Communication Resources for Pediatricians
CDC Health Advisory – Outbreak of Pseudomonas aeruginosa
Health Alert Network
Human Parechovirus (PeV)
Maryland Morbidity Report Form
Measles Vaccinations
Tuberculosis
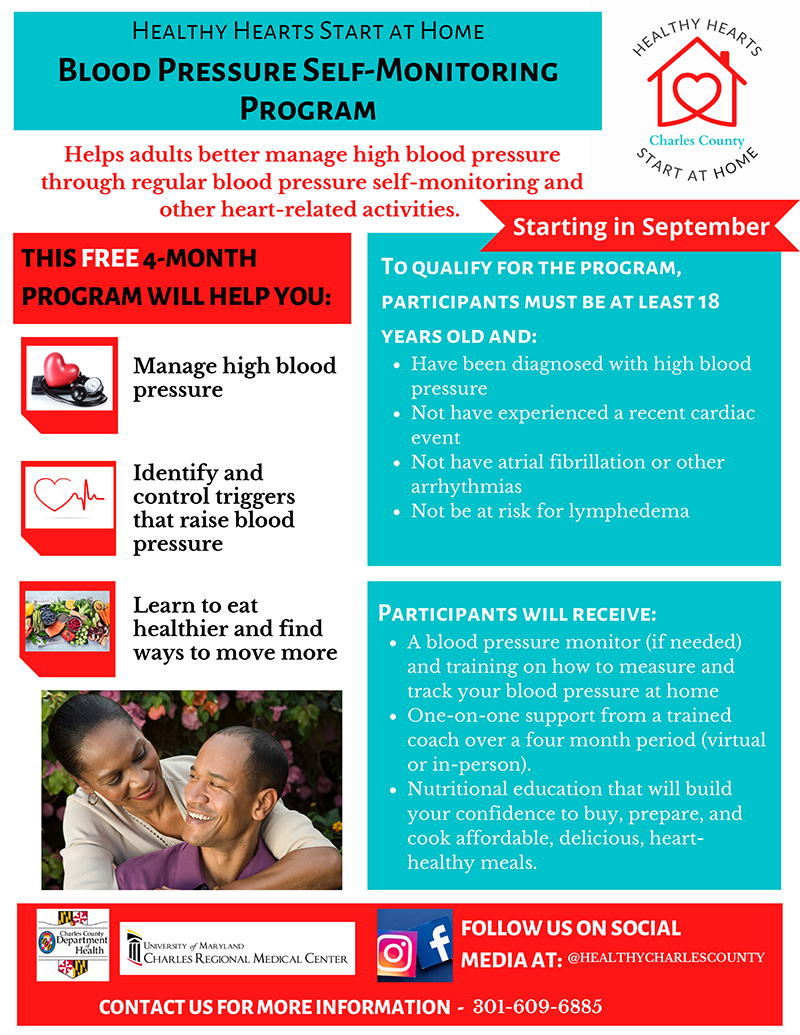
Healthy Hearts Start at Home
Healthy Hearts Start at Home
Please complete this enrollment form if you want to participate in the four-month blood pressure self-monitoring program.
Healthy Hearts Start at Home
"
*
" indicates required fields
Email
*
Name
First
Last
Telephone Number
Date of Birth
*
Month
Day
Year
Sex
Male
Female
Other
Were you diagnosed in the last 12 months with high blood pressure/hypertension?
Yes
No
Are you on medication to control your blood pressure?
Yes
No
Do you have Atrial Fibrillation (A fib) or other Arrhythmias?
Yes
No
I don't know
Do you have or are at risk for Lymphedema?
Yes
No
Have you experienced a recent cardiac event within the last 12 months?
Yes
No
I don't know
How would you classify your current activity level?
Low Activity
Moderate Activity
High Activity
How often do you use alcohol?
1
2
3
4
5
1 For Often and 5 for Never
How often do you use tobacco?
1
2
3
4
5
1 For Often and 5 for Never
How often do you use caffeine?
1
2
3
4
5
1 For Often and 5 for Never
Do you have a computer and internet access?
Yes
No
How often do you use recreational drugs?
Often
Never
Do you currently have a working blood pressure monitor at home?
Often
Never
What is your current weight?
Weight in KG
What is your current height?
Height in CM
Is there anything else you would like us to know?